Challenges for Ethical Humanitarian Health Responses in Contemporary Conflict Settings

This essay examines the pressures and narratives that constrain humanitarian health actors from meeting their commitments to ethical conduct. I focus on critical contemporary issues that exacerbate or generate new ethical concerns for humanitarians, such as the imperatives to be accountable to affected populations, to “decolonize” humanitarianism, and to respect intersectional diversity; and how maleficence should be interpreted in this changing context. I argue that by adopting certain practices—particularly those that create space for new voices and confront entrenched power systems—today’s humanitarian health actors can remain true to their core ethical principles.
Humanitarian principles are a set of values designed to guide decision-making in the face of limited resources, competing interests, and ethical dilemmas. Humanitarian actors are expected to both operationalize and embody principles as a kind of moral code to navigate the complexities inherent in mounting an emergency response in areas where one is required. By referring to these principles, humanitarians are validating the sector’s ethical boundaries and distinguishing themselves from other interveners who, while providing similar services, may embrace different ethical frameworks. Beyond their moral origins, humanitarian principles can also be instrumental in enhancing the security of humanitarian actors on the ground and ensuring their access to populations in need. Humanitarian principles can thus be seen as key enablers for successful humanitarian operations, serving both as an overarching moral framework for action and a basis for pragmatic responses to humanitarian crises.1
Ethical Principles Guiding the Humanitarian Health Response
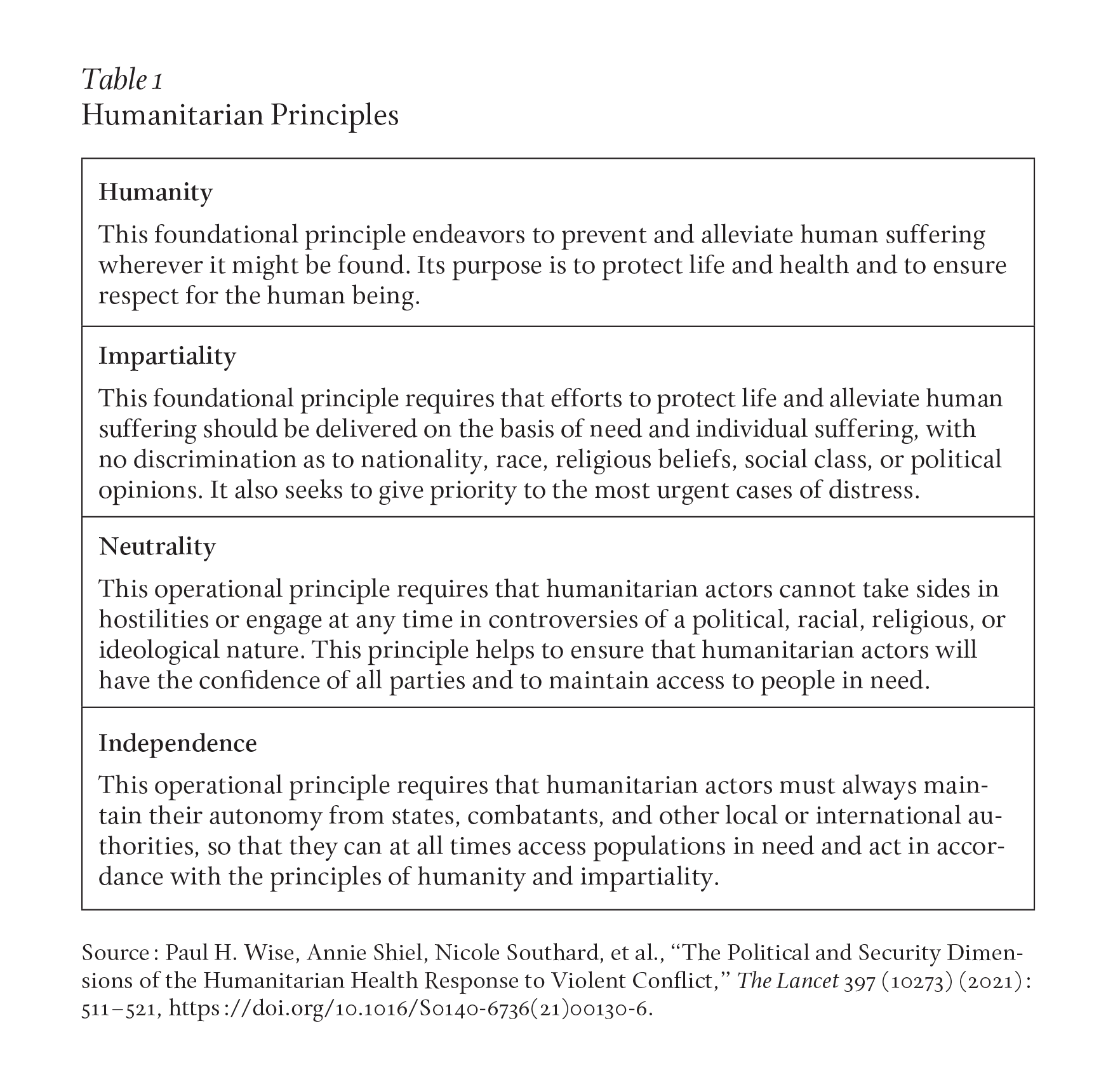
There are four central principles that underpin contemporary humanitarian action in settings of conflict: humanity, impartiality, neutrality, and independence (see Table 1). Although some humanitarian organizations may add other guiding principles, these four constitute the core of what has been called the “Dunantist tradition” in Western humanitarianism, named for Henry Dunant, one of the founders of the International Committee of the Red Cross.2 Given our focus here is on humanitarian health responses, there are other principles that are particularly relevant to the delivery of health services, including a respect for the dignity, agency, and autonomy of the individual receiving care, to ensure benefit to those receiving an intervention, to avoid harm (nonmaleficence), and to commit to the just application of resources. More broadly, humanitarian health personnel are expected to respect medical ethics in their daily work.3
Even if these additional elements have not been explicitly framed as part of the guiding principles for humanitarian health provision, they have in practice been incorporated into the strategies and normative doctrine of humanitarian health actors.4 In this way, the ethical framework guiding humanitarian health responses can be seen as broader than that which shapes other forms of humanitarian assistance.5 For example, nonmaleficence—which is commonly interpreted as “do no harm”—might not be traditionally labeled as a humanitarian principle, yet there is little doubt that it has a prominent place in the hierarchy of effective concerns shaping humanitarian health. Other important examples include the just distribution of resources and the preservation of confidentiality.
In focusing on this broader set of principles and the contemporary context for their application, this essay takes a practice-facing rather than conceptual approach. More specifically, it highlights some of the emerging issues that are currently circulating in settings of humanitarian health response. These include “accountability to the affected population,” “decolonization” of humanitarianism, “intersectional diversity,” and the evolving interpretation of maleficence. The essay concludes by pointing to some new practices that can ensure that humanitarian health responders remain true to both humanitarian and medical ethics, especially in highly dynamic political and security environments.
Emerging Challenges to Traditional Humanitarian Principles
In recent decades, humanitarian organizations have had to confront pressures generated by a rapidly changing operational and political context that demands that they commit to taking concrete steps to strengthen accountability.6 Although some of these pressures may not be entirely new, their effects on humanitarian health responders have become more consequential in recent years.7
For example, the growth of digital media and their utility in conflicts and crises have increased the scrutiny of humanitarian decision-making. Humanitarian funding has increased globally, creating new actors and expanding response capacity. New technologies and digital tools are developed and implemented at full-speed, as the humanitarian sector struggles to keep up with the inclusion of protective digital safeguards. A further example is the proliferation of conflict actors and the intensification of asymmetric warfare, which have contributed to a far more complex humanitarian landscape in which command and attribution have become more difficult to discern. Moreover, the protracted nature of conflict and the contemporary emphasis on a “humanitarian-development nexus” implies a continuity of response that can challenge the traditional boundaries between neutral and independent humanitarian action and non-neutral development partnerships, often with the engagement of states.8 Finally, the urgent consequences of climate change and growing concerns around sustainability now frame the daily dynamics of humanitarian health responses.
There is also a set of justice-related challenges that calls upon humanitarian health actors to rethink the way they operate. New commitments to equity, diversity, and inclusion—which previously garnered little attention in humanitarian action—are now raising questions about the colonial roots of global humanitarian structures and how power is exercised through humanitarian interventions. These concerns have grown in demands for “localization,” which emphasizes the importance of bottom-up and participative approaches in humanitarian activities and primary accountability to local populations, as opposed to donors. More broadly, a greater appreciation of planetary health has also raised important questions about traditional humanitarian health ethics and practices. The preservation of natural ecosystems and the well-being and recovery of the environment must also be incorporated into the fabric of humanitarian practice.9
The core humanitarian principles of humanity and impartiality compel the relief of suffering based on need, and yet there is a growing imbalance between “forgotten” or “invisible” crises and those that are elevated by donor preferences and Western media. Moreover, targeted legislation or sanctions as well as the shifting priorities of the UN Security Council can enhance or diminish humanitarian action in specific settings around the world. The prioritization of certain health needs and the neglect of others may also reflect external pressures rather than the careful application of traditional humanitarian principles.
The principle of independence can also be challenged by external pressures. While this humanitarian principle calls for autonomous decision-making by humanitarian organizations, specific, earmarked funding or the preferences of host states can impose targeted uses of resources that does not always correspond to observed needs or gaps in service provision.10 Ethical decision-making entails efforts to ensure that local communities and civil society have opportunities for shaping the local humanitarian agenda. However, this may chafe against the need to remain independent, particularly when local communities are closely affiliated with a particularly political or combatant group.11 At the same time, any stakeholders’ interests must always be weighed against the imperative for health care providers to be first and foremost responsive to the wishes and needs of the person receiving health care. Given the complexities inherent in navigating this array of influences, humanitarian organizations may rely on transparency in operational decision-making to convey how they attend to the requirements of ethical humanitarian principles.
Respect for Local Voices
The imperative for humanitarian actors to acknowledge the voices and priorities of communities has ascended to an increasingly prominent place in the contemporary humanitarian agenda. While this practice can sometimes create ethical dilemmas, particularly in remaining independent and neutral, it can also be viewed as a way of strengthening ethical decision-making. Diverse communication channels, including traditional community gatherings as well as social media engagement, can expose humanitarians to community views and facilitate joint delineation of the priorities for the humanitarian health response. While there is often a mismatch between the community’s ask and the proposed response from humanitarian health actors, this can lead to essential conversations and help ensure that humanitarians act as true “responders” and not as “interventionists.”12
Although this dynamic is often depicted as humanitarian actors enhancing their “accountability to the affected population,” this expression can unwittingly create the impression of an us-versus-them dynamic that overlooks the possibility of local communities and humanitarian organizations codesigning humanitarian health responses. This latter practice, if fully incorporated into humanitarian work, could potentially have a profound impact on strategic and operational decision-making. More specifically, it could shape new ethical approaches to humanitarian health in which neutrality and impartiality are in large part defined by communities that, in their empowered role, seek to defend their interests beyond the limits of what may have traditionally been deemed acceptable by humanitarian organizations.
At the same time, greater care and attention need to be paid to the potentially counterproductive role that social media can play in ongoing exchanges between local communities and humanitarian organizations. The proliferation of misinformation or disinformation calls for transparent and frank dialogue between humanitarians and other stakeholders, especially those who represent the communities that humanitarian organizations wish to serve.13 Humanitarian principles themselves should form a core foundation for this dialogue, a commitment that requires a willingness from all parties to collaboratively explore the ethical standards that humanitarian organizations are seeking to operationalize. While, under some circumstances, this dialogue can expose difficult tensions between humanitarian organizations and community members, the transparent exploration of these issues can identify conflicting, even abusive attitudes regarding impartiality, independence, and neutrality. It can also provide a conducive platform to foster trust and ultimately joint compliance with a common set of ethical protocols and procedures.
Humanitarian Ethics and the Exercise of Power
Beyond the demand for greater attention to diverse voices, discussions about the decolonization of humanitarian health responses have had to confront the implications for the principle of nonmaleficence, the obligation not to inflict harm while providing care. This justice-related claim contests the status quo distribution of power and speaks directly to how humanitarian health responses are designed, delivered, managed, and evaluated. From an ethical point of view, calls to decolonize humanitarian health responses raise the fundamental question of what values and purposes humanitarian principles serve if they are not confronting the inequitable distribution of power, knowledge, and resources in the humanitarian space.14
The humanitarian sector seems to be alarmed by the prospect that their practices might, in fact, be strongly rooted in colonialism. From an ethical standpoint, acknowledging these colonial origins means more than debating constructs that relate to compliance with traditional humanitarian principles. It also entails deeper questions about the future of a sector that was established, governed, and driven by Western, and largely white, institutions.15
The issues around inequality and power imbalances reflect a lack of diverse representation in strategic decisions, recruitment strategies, the establishment of salary grades, the management of discrimination and abuse, and the targeting of specific health problems and populations. Of particular concern to humanitarian health, power imbalances can distort therapeutic choices, the types and origins of employed drugs and medical devices, and supply channels for a variety of essential humanitarian materials. These issues may raise questions beyond humanity, impartiality, neutrality, and independence. But can humanitarian provision be truly ethical if these problems are not addressed?
While localization has been embraced as a remedy to counter some of these power imbalances, its comprehensive implementation remains rare. In addition, the full utility and limits of localization will vary in different social and political settings.16 While the goals of many humanitarian organizations might aspire to meaningful inclusiveness and diversity, achieving these goals will likely require a deeper revision of long-standing values and a willingness to challenge practices established in a colonial past.
Even the language of humanitarian health requires ethical reassessment. Affected communities are often described as “beneficiaries,” “recipients,” or “victims,” which tends to diminish community strengths and, more profoundly, community power. Language is a battlefield of ethical reality and should also be the subject of collaborative reflection and revision.17 Public communication and “marketing” shaped by the interests of the organizations can prove disrespectful of communities and their dignity, and instrumentalize human suffering. Humanitarian organizations are often engaged in intense data collection protocols, yet the discussion of consent regarding the use and storage of data, particularly using digital technologies, may not meet ethical or humane standards.
Most important, humanitarian principles, particularly the principle of neutrality, should not be used as a shield to community engagement or to avoid unpleasant conversations about inequalities and the abuse of power. Rather, ethical considerations should support the thoughtful yet forceful protection of communities and actively work to use humanitarians’ own base of power to challenge inequalities, give space to diverse voices, and actively promote change.18
Identity and Intersectionality in Humanitarian Health Responses
Humanitarian actors today face new demands to ensure that the identities of individuals and groups are respected in the design and delivery of humanitarian health responses. Intersectionality is “a way of thinking about identity and its relationship to power,” and emphasizes that people’s lives are shaped not by a single factor but by a variety of personal, political, and social dimensions.19 It thus seeks to identify the many ways and forms in which a person can be or become powerful and be or become susceptible to abuse or invisibility. Intersectionality reminds humanitarian health workers that the traditional mindset of “risk groups” might be imperfect or simply too reductive to facilitate just humanitarian action. Embedding intersectionality within the guiding ethical principles for humanitarian action would therefore mean, first and foremost, that the humanitarian sector must identify its own limitations and biases that necessarily frame its approach to each context.20 Humanitarian actors are often unaware of, or understate, the impact that operational mandates, international guidelines, or legal frameworks have on their understanding of and response to the challenges in distinct humanitarian settings.21
There is still much to be done to expand new practices that respond to justice-related claims. There is a need to embed them more firmly within both the humanitarian sector’s conception of ethical action and its everyday implementation on the ground. This will surely require ongoing critical dialogue, and the humanitarian health community must reassess its ethical foundations that, while controversial, could provide guidance for a range of ethical realignments in the humanitarian response and patient-centered care.
Ethical principles exist because reality can be messy, confusing, and contradictory. Solutions to such challenges will always be less than ideal, and it is unsurprising that the just application of ethical principles would be similarly complex. However, complexity should not be used as an excuse for inaction. In this context, it should be remembered that the ethical principles of humanitarian health are principles of action intended to motivate and facilitate deeds in the real world.22
There is also a constant need for reassessing the translation of ethical principles into action, particularly in an area as dynamic as humanitarian health. There is a requirement for listening and responding and not the veiled imposition of unilateral declarations or positions. Enacting principles in a complex, fast-evolving environment means that humanitarian health workers should be capable of critically reflecting on their practices and ensure that their choices are relevant to and respectful of the communities to be engaged. Principles in action are people-centric; they should first and foremost respond to the benefit of those whom the humanitarian sector intends to support.
Throughout this essay, I have emphasized the need to create and strengthen participatory and representative platforms of conversation as a way to keep humanitarian principles alive, relevant, and actionable. Many humanitarian health organizations are actively engaged in seeking new ways to address these challenges through reflection, facilitated engagement, and action. I have also advanced the argument that humanitarian health workers who directly deliver services to communities in the field are essential guides to the deliberation of ethical frameworks. Finally, I have underscored the necessity that humanitarian organizations invest in attitudes and practices that open space for the voices of all those engaged in health responses and to actively break down power structures that stress or create vulnerability and impotence. This more expansive commitment will best ensure a constructive rethinking of the ethical basis of humanitarian health, and ultimately prove sufficiently insightful, actionable, and humane to meet the rapidly changing reality of humanitarian health in the real world.
author’s note
This essay does not represent the views of the International Committee of the Red Cross, where the author currently works. The author wishes to thank Lina Echeverri, Mutsa Mugangavari, Maria Guevara, and Berhanu Endeshaw, who generously offered feedback on earlier drafts.