Localizing the NGO Delivery of Health from the Outside In

International health nongovernmental organizations (NGOs) can provide the necessary assistance and expertise to save lives in times of crisis. Health NGOs often bring innovation, expertise, and resources to those in need. However, many commentators have questioned whether the involvement of health NGOs impedes a country’s ability to rebuild its own health sector in ways that do not depend on foreign actors. Building on the results of our survey of almost one thousand public health NGOs in the summer of 2021, we find that health NGOs may be a unique set of organizations that allow for more local decision-making and employ local staff more often than other populations of NGOs. Health NGOs also have a comparatively greater focus on peace than NGOs from other sectors. The essay examines the pathways by which some health NGOs can both alleviate short-term suffering and help foster long-term localized health delivery.
International health nongovernmental organizations (NGOs) could be the ideal provider of health services in conflict and postconflict areas. When adequately funded, international health NGOs can deploy quickly to an affected area, bringing much needed expertise and supplies. If international health NGOs can partner effectively with local actors, existing case study and anecdotal evidence suggests that they could help provide long-term solutions to health care and build capacity in postconflict countries.
Despite their tremendous potential, we still have relatively little specific data on health NGOs. To our knowledge, there is no systematic, cross-national study on whether health NGOs improve localized health outcomes in postconflict societies, and no current data set provides the information that would be necessary to carry out such a study. While scholarship on NGOs has increased in the last twenty years, most of the focus within international relations still remains on organizations that specialize in human rights or environmental advocacy.1 Even recent efforts to collect data on humanitarian actors leave out the work of health-specific organizations.2
Before we can further substantiate the increasingly vocal arguments about localization in postconflict health delivery, we need to better understand the characteristics and behavior of the international NGOs often acting as a conduit for health services in fragile areas. We need more information on the unique qualities of health NGOs, especially at the intersection of health and conflict. Further, drawing on recent discussions on the importance of localization, sustainable health delivery requires us to better grasp the efforts these health NGOs have taken to localize health services and build critical domestic capacity.
This essay is one small step in that direction. We surveyed 2,495 international NGOs, one-third of which could be categorized as health NGOs. We examined their broad interests and their efforts at localization, comparing the sector as a whole with non-health NGOs. Our findings show that health NGOs may be a unique set of organizations that allow for more local decision-making and employ local staff more often than other populations of NGOs. Health NGOs also have a comparatively greater focus on peace than NGOs from other sectors. Our survey and results are thus important steps in better understanding the whole health NGO sector and its unique capabilities for localization and sustainable service delivery.
What We Know about the Work of Health NGOs
Health NGOs technically include everything from not-for-profit hospitals to organizations that focus only on advocating for a specific health policy or affected population. In this essay, we focus mainly on international NGOs—defined as those organizations that are operating in countries other than their base or headquarters country—that self-identify as having a focus on public health. Médecins Sans Frontières (Doctors without Borders), Imamia Medics International (IMI), and International Medical Crisis Response Alliance would all be categorized as international public health NGOs. Additional examples of health NGOs include faith-based organizations such as Hospitals of Hope, American Jewish World Service, Samaritan’s Purse, Medair, and Cure. Other efforts include more regional-specific health NGOs that are privy to tight networks of volunteers who are able to deploy for service with little to no prior notice.
Numbering in the thousands, health NGOs can act as a stopgap when government and for-profit health services are destroyed, often working to establish lasting public health programs as countries rebuild.3NGOs are nimble and bring specialized knowledge built on extensive experience. When compared with other potential suppliers of health services in the aftermath of conflict, like peacekeepers or foreign military interveners, health NGOs often bring less political baggage, and as a result, these organizations may be able to reach rebel-held populations that could prove dangerous for armed interveners.4
There is no one dominant approach for international health NGOs; organizations work in a variety of different ways. This variation is illustrated in Figure 1, drawn from our survey (which we elaborate on further below). As shown, while many health NGOs focus on service provision and program implementation, some organizations are also involved in advocacy, capacity-building, and research.
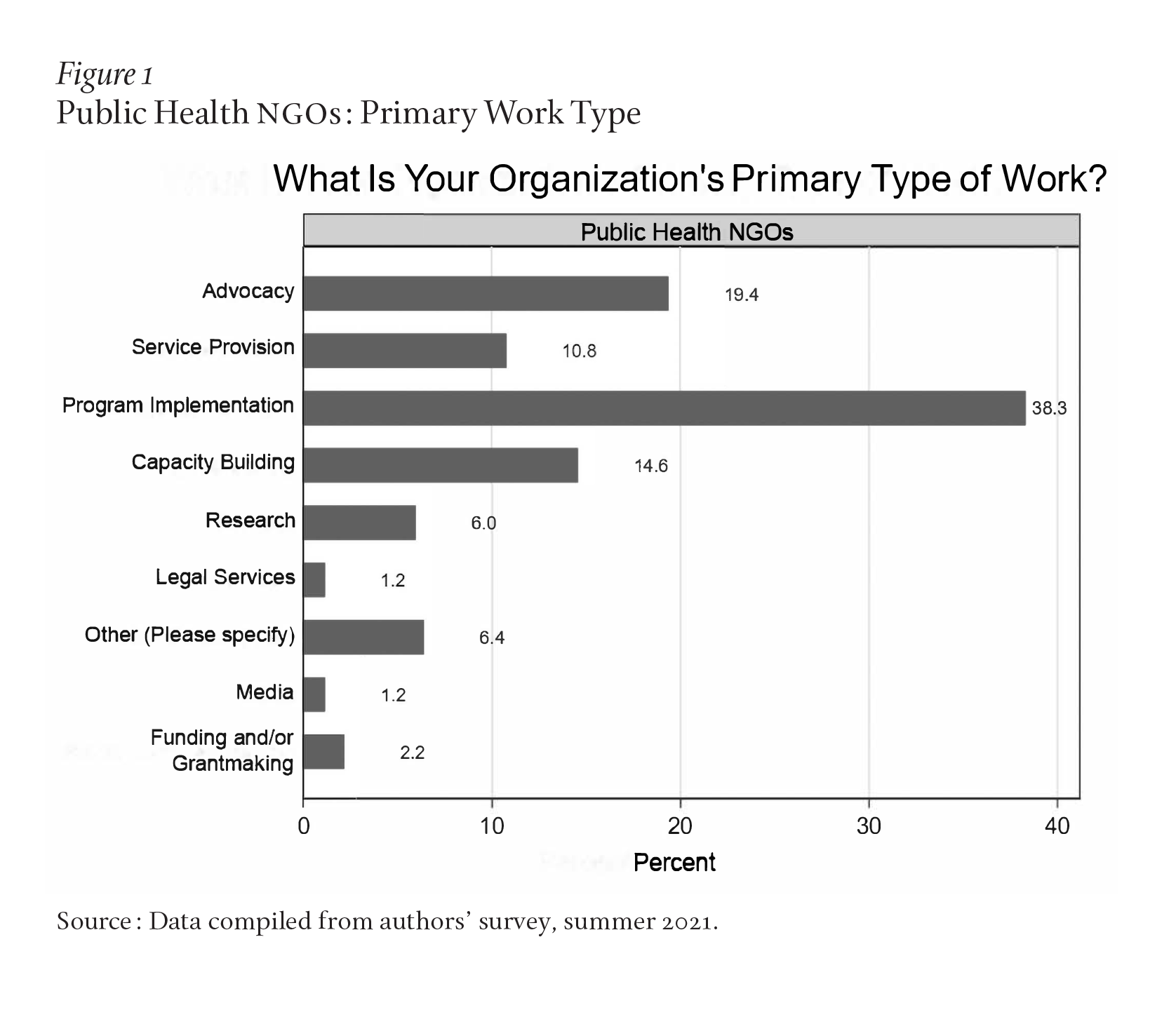
Even among the set of health NGOs focusing on program implementation and service provision, organizational tactics and approaches vary. Many organizations carry out services themselves using a combination of both local staff and international volunteers and employees. International health NGOs are also often involved in the training and equipping of local health providers. Some of these NGOs directly interface with governments on reforms and improvements to public health systems.5 Some organizations also work to educate populations on vaccine efficacy, nutrition, or other public health concerns.
Issues of Localization for Health NGOs
While the activities of some individual health NGO efforts may be short-term or narrowly defined, like helping to coordinate cleft palate repair in a specific location over a two-week period, for example, other health NGO efforts involve a longer-term commitment and provision of a broad portion of a location’s health services. For example, as political scientists Abdallah I. A. Yagub and Khondlo Mtshali’s interviews of health NGOs in North Darfur in the early 2010s showed, at that time, international health NGOs were “providing 70 percent of curative health services to the State’s population by contributing 52.9 percent of the health budget and 1,390 health personnel.”6
However, such NGO dominance in health care provision within a country is not ideal. For decades, there has been widespread concern that international NGOs that provide health care services will erode government initiative and harm a local population’s expectations and respect for the domestic political system. As one commentator put it, NGOs could eat away “all the flesh of the state.”7 By providing services themselves, NGOs might help their own longevity, but they might also create cycles of dependence that could ultimately harm sustainability and local capacity. However, despite concerns to the contrary, no health NGO has the goal of taking over state roles.8 In fact, transitioning from a health system that is NGO-dependent to a more sustainable, locally led public health system is the more typical objective of international health NGOs.9
Discussions of the importance of local capacity and buy-in have increased in recent years, spurred on by the World Humanitarian Summit in 2016. Localization is defined broadly as efforts intended to move international aid away from international donors and large NGOs and direct the aid more toward local and national civil society.10 Among the many commitments to localization is a goal of at least 25 percent of humanitarian aid going directly to local or national actors.11 Localization efforts have previously been justified on both moral and effectiveness grounds.12 Morally, localization works to address power dynamics and legacies of colonial repression. From an effectiveness perspective, localization helps to build community trust, support, and buy-in, which limits “brokerage” costs or the role of so-called middlemen. Localization as discussed and agreed to at the 2016 World Humanitarian Summit was not entirely new, and many have remarked on how local capacity building and service delivery have been aid goals for decades.13 Many international NGOs have already adopted a hybrid local-international approach to program design and delivery.
There have also been some arguments against localization, especially in times of conflict.14 International organizations may have both the capacity and the neutrality that national or local organizations could lack during a conflict. There are also concerns about the potential for localization to create increased risk for local staff, while international actors remain on the sidelines.15 Nonetheless, the ongoing discussions about localization have led to an increased focus on the need for locally informed decision-making and staffing. Local ownership, training, and decision-making may be especially important in the postconflict stage, as the aid returns from bypassing state actors and governments increase their capacity to carry out health services in peacetime.16
Obstacles for Health NGO Effectiveness
There are many obstacles to the work and effectiveness of health NGOs, even in peacetime. For example, organizations often do not coordinate with each other and with other government and international efforts that are also aimed at reducing suffering.17 Health NGOs are often operating within an aid framework that fosters competition with one another in order to ensure their own organizational survival.18 This lack of coordination can harm collaborative efforts, leading to an overabundance of resources in some locations and a lack of resources in others.
The possibility of rapid changes in funding streams also harms the work and effectiveness of international health NGOs. Donations can be redirected to the “next big disaster,” often leaving organizations scrambling to change their portfolios.19 The nature of their funding stream can also influence their work. If funded by foreign governments, for example, NGOs may lose access to certain populations and could be seen as political agents.20
Government and intergovernmental organizational funding may nonetheless be required for the broad scope of the health concerns needing to be addressed; local, individual contributions simply may not be enough to address the needs of a crisis-affected population. In this context, some local governments may view NGOs as competitors for aid funds, especially if foreign donors are channeling aid to NGOs that had previously been directed at national governments.21 The aid environment, together with the quickly evolving conditions in conflict- and natural-disaster locations, may lessen the ability of NGOs to carry out their own research on what works and may increase concerns about the need for organizational monitoring and accountability.22
A further challenge is the potential for “voluntourism,” which often involves NGO staff engaging in short-term volunteer efforts for personal gain or self-fulfillment.23 Voluntourism may result in a myriad of negative effects for local populations, including re-traumatization, abuse of life experience for NGO fundraising efforts, or the misuse of the volunteer’s name/likeness for the sake of NGO marketing campaigns. Scholars have raised concerns about international health service trips involving students, during which local individuals often feel that their preferences are ignored and that populations served by volunteers receive lower quality of care due to lesser-skilled volunteers.24 Using international aid as a platform for training or other related student activities commodifies local populations and suppresses the ongoing work of local NGOs and more locally engaged international NGOs. While many health volunteers operating through NGOs may initially have altruistic motives, their presence has in some cases resulted in tragic consequences and even death. One pertinent example of this occurred in Jinja, Uganda, where Renee Bach faced charges for allegedly faking her identity as a medical professional when opening a health NGO, an action which resulted in the deaths of multiple children.25
Health NGOs are also concerned about their own safety and longevity, both for their staff members and volunteers and for the organization as a whole. NGOs must attend to the potential risks to their ongoing work, including the personal safety of their volunteers, and their ability to both secure funding and avoid repression efforts by local governments. In carrying out public services, workers from international health NGOs can be targeted by crime and political violence, both in times of conflict and during peacetime.26 Even neutral health NGO workers may be mistaken for peacekeepers or foreign military interveners, thereby placing them at greater risk.27 As risks increase, organizations face difficult choices and often must make compromises in the quality of care and in the safety of staff members.28
Taken together, trends such as these have contributed to a more general backlash against foreign-funded NGOs over the last twenty years, with organizations being kicked out of countries where they previously had long-term cooperative service-delivery arrangements.29 When allowed within a country, international health NGOs have seen an increase in restrictions and host government oversight. While some of these restrictions may be justified by the regime to help curb corruption, protect against terrorism, or otherwise deal with some of the shortcomings in the sector discussed above, many of the limitations on NGO operations are part of a larger trend of democratic backsliding and human rights abuses.30 International NGOs are increasingly being associated with Western interference and attacks on state sovereignty, which could lead to a populist backlash against even local civil society actors.31
All of these challenges, which are endemic to the health NGO system, are compounded in times of conflict. Attacks on aid workers increase with the severity of the conflict.32 Concerns about safety may lead to international health NGOs fully halting operations or moving their operations across a border, which can also complicate health care delivery, coordination, monitoring, and trust.33 Local health workers may also flee the conflict zone, making it more difficult for international health NGOs to find local partners and staff. Nonetheless, we do know that organizations still provide necessary health services in times of conflict and often aid in rebuilding health services in the aftermath of conflict. Some international health NGOs work directly with populations harmed by the conflict, setting up field hospitals and triage centers as in Syria, for example. Other NGOs may continue to work on communicable diseases or their non-conflict health-related missions. And some organizations manage to negotiate access to provide these health services in rebel-held areas and advocate for health-related ceasefires. For example, UNICEF and the Catholic Church helped to create a widely praised ceasefire that allowed for childhood immunization in El Salvador in 1985.34 The Carter Center negotiated a ceasefire with the Sudan People’s Liberation Army for aid workers to help treat populations affected by Guinea worm disease and river blindness in 1995.35 Although not always successful, organizations are currently negotiating with rebel groups for COVID-19 vaccine distribution, despite deep mistrust of foreign interveners of any type.36
As fighting ends, health NGOs may be the only option for starting to rebuild health services. On the positive side, there is large-scale evidence that health NGOs are successful in reducing infant mortality in developing democracies.37 Evidence shows that the activities of international health NGOs also lead to an increase in government spending on health care provisions, an outcome that helps to illustrate that international NGOs do not harm a government’s incentive to provide their own health services and may increase demand for public health measures.38 In fact, international health NGOs often try to partner with governments, hoping to help transition a country from dependence on external health services to a fully functioning government public health system.39 The quality of these partnerships varies, with some governments seeing NGOs as an untrustworthy competitor for aid funds.40 Regime leaders in democratic governments may have more incentives to partner with international NGOs and transition to providing bureaucratic services themselves, since widespread electoral support is critical for their own political longevity.41 Recent experimental research also finds that international NGO projects may increase the public’s approval of the government, calling into question concerns about potential deleterious effects of NGO-provided services on government initiative and state-society relations.42
Urgent Need for More Information on Health NGOs
As the studies discussed above illustrate, international health NGOs could be a key solution for health and human security, even in conflict and postconflict situations. However, there are many ongoing issues with the sector, including concerns about a lack of local capacity-building and local buy-in. To our knowledge, there is no data source that would allow us to examine both the problems and conditional effectiveness of health NGOs on a broad, cross-national scale.
In the summer of 2021, we used a survey approach to collect new NGO data, through an original email survey of more than thirty thousand NGOs that constitutes one of the first cross-national, global surveys of NGOs. We tried to be as inclusive as possible in our list of possible recipients, using organizational email addresses listed in the UN’s integrative Civil Society Organizations (iCSO) System and other publicly available websites and organizational contacts.43 We received 2,495 responses to our survey. Of those organizations, 845 reported that they had a focus on “public health.”
Our survey asked eighteen questions, focusing on organizational-level activities and functions, which allows us to refer to respondents as “organizations” throughout. The survey questions included a variety of demographic-related topics, such as founding year, headquarters location, staff sizes, and funders. In addition to the demographic information, we also included questions focused on each organization’s type of work, collaborators, organizational decision-makers, framing decisions, meeting attendance, and issue focus.
Our survey data will be helpful for researchers interested in addressing many of the unanswered questions about the nature and behavior of contemporary health NGOs. Here, we focus specifically on the results of the survey that will improve our knowledge about the current work of health NGOs in regard to localization and peace.
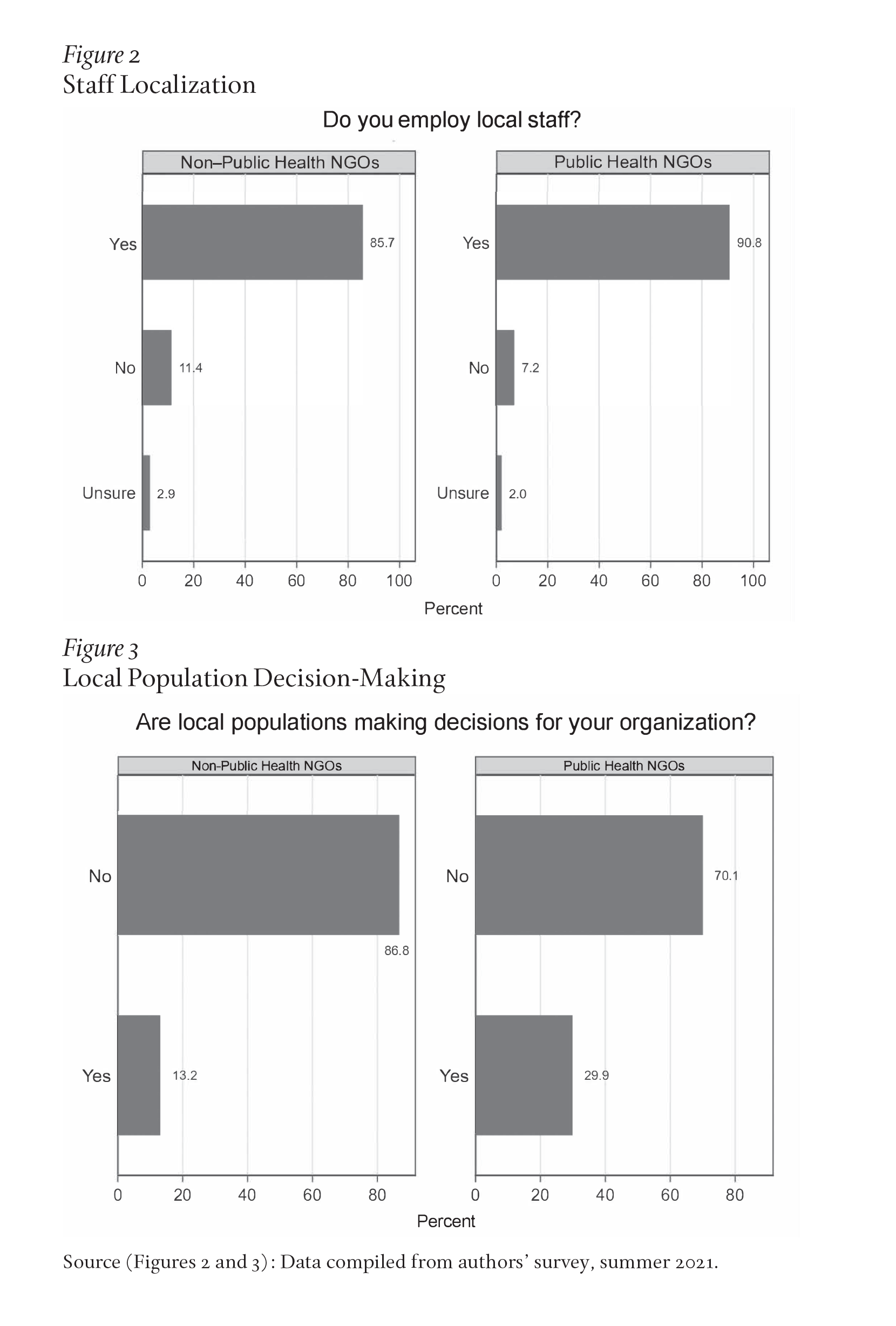
First, there is evidence that international health NGOs are acting somewhat more consistently with the goals of localization than organizations without a health focus. As Figure 2 shows, 90.8 percent of health NGOs report that they employ local staff. A χ2 test (or chi-squared test) allows us to conclude that this is statistically distinct from the lower 85.7 percent of local staff employed by other types of NGOs.
Even when employing a high percentage of local staff, however, it appears that international health NGOs, like the broader population of NGOs, still do not routinely involve local populations in their decision-making. As seen in Figure 3, roughly 70 percent of public health NGOs reported that local populations are not making decisions for the organization. This is statistically distinct from the 87 percent of non–public health NGOs that also report not having local populations make decisions for the organization. Taking these figures together, it does appear that there are some localization efforts currently being undertaken by NGOs, especially by public health NGOs, although the general levels of localization may be far from the ideals set out by the 2016 World Humanitarian Summit.44
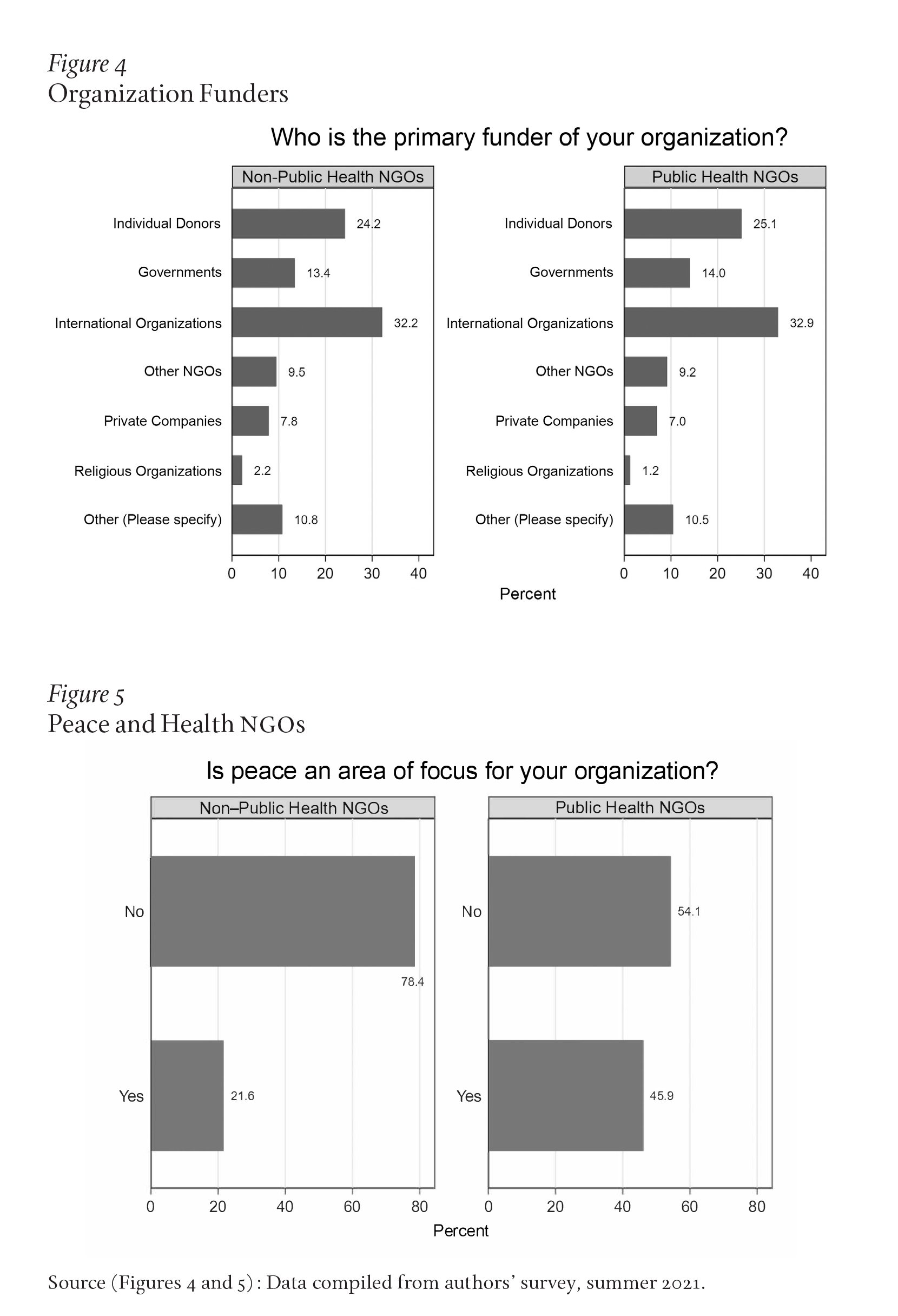
The less-than-ideal localization efforts may be a function of the funding structure. As shown in Figure 4, when organizations are asked about their funders, the largest group of NGOs report that they are primarily funded by international organizations. There is no statistical difference in funding sources between public health and non–public health NGOs. This information could suggest that any additional attempts at increasing local decision-making may need to be led by international organizations and further incorporated into their funding requirements.
Unfortunately, as our survey was general, we did not ask participating organizations any questions about their involvement in armed conflict situations. However, organizations were able to indicate multiple areas of focus in their responses, including a focus on “peace.” No definition of peace was given in the survey itself, but organizations were able to indicate whether this was one of their focal areas. As Figure 5 shows, we did find that public health organizations were much more likely to report that they also had a focus on peace than non–public health organizations. This relationship is statistically significant, as determined by a χ2 test.
Our collected data demonstrate the need for more surveys of health NGOs, specifically on ideas around conduct during and after conflicts. How might health NGOs uniquely serve in the peacebuilding process? What is the relationship between health NGOs and other important stakeholders on the ground who are also actively involved in the peacemaking and peacekeeping process? How do health NGOs relate to UN peacekeepers and other NGOs focused on other conflict-related issues? How do health NGOs view local populations and localization efforts? Do opinions of localization shift in times of conflict? These questions may be best answered through survey research focused on NGOs, their activities, and priorities.
A Way Forward
International health NGOs are a critical link in public health, and we are just beginning to fully grasp the processes by which they could affect both short- and long-term solutions in conflict and postconflict areas. Already difficult NGO work is made even more challenging by fears of violence. While problems with the sector undoubtedly exist, earlier concerns with NGOs leading to a lack of government initiative or investment or changes in state-society relationships appear to be overblown. Newer research indicates that national governments can benefit from international NGO service provision and that NGO partnerships may help governments invest in public services and improve their own capacity and legitimacy.45 These results are general, however, and more emphasis on how armed conflict dynamics could complicate these trends is necessary. Efforts at localization, both during conflict and in peacetime, should also be examined in more detail.
We have argued here that data collection efforts are a crucial part of improving health NGO service delivery. Rigorous program evaluation and analysis are necessary to understand the impact of health NGOs’ efforts and the consequences of their decision-making processes. Otherwise, there remains the risk of harming local populations by the efforts designed to initially improve quality of life. Our research thus points to the need for heightened investment by academics and policy-makers alike into understanding the particular mechanisms and predictors of localization of health NGOs in various contexts. Outcomes vary depending on the country of focus, so further case study work on this topic would help us understand which strategies work best depending on where they are located.
While survey research of NGOs is an important step in this process, we would also recommend investment in public opinion research on health NGO services and efforts. We need to better understand how recipient populations think about health NGOs and whether they see a way forward that empowers local actors and community needs. One of the frequently overlooked aspects of research is prioritizing the participant experience, whether due to lack of access to these respondents or ethical concerns—all of which create roadblocks to accurate information. These challenges demand creativity from the academic community and NGOs alike to assess the needs of local populations without placing undue burden on respondents. By increasing efforts to improve the impact of localization on health NGOs during times of peace and conflict, NGOs can better prepare for the future and best allocate resources to proficiently serve some of the world’s most vulnerable populations.