The Missing Piece: A Population Health Perspective to Address the U.S. Mental Health Crisis

The COVID-19 pandemic has enhanced our focus on mental health. Concerns about the high levels of mental disorders in the United States are not new, with rising trends–particularly among youth–observed prior to the pandemic. However, the pandemic may have exacerbated and accelerated these trends. The silver lining is that we can leverage this moment to reevaluate and reimagine not only how we treat mental health problems, but also how we promote emotional well-being throughout the life course. We argue that scholars, policymakers, and practitioners should broaden their view of mental health, and consider it as a full spectrum ranging from serious mental illness to robust emotional well-being. This perspective recognizes the importance of treatment access and quality, but also elevates the value of prevention, particularly at the population level. Greater attention to preventing problems before they occur will not only reduce manifest disorders but also encourage higher rates of psychological resilience and, ultimately, better physical health.
The COVID-19 pandemic has focused greater attention on mental health in the United States and has driven renewed interest in the effects of social and psychological experiences such as isolation, loneliness, stress, and uncertainty on emotional well-being. However, even before the pandemic began, the number of people in the United States experiencing mental health problems was high and on the rise, particularly among young people. In fact, the high prevalence—or overall proportion—of mental disorders in the general population of the United States has been recognized for decades, documented first in the Epidemiologic Catchment Area Survey carried out in the 1980s and confirmed in the 1990s with findings from the National Comorbidity Survey.1 These studies and many others conducted prior to the pandemic demonstrated that at least one in five Americans suffers from a mental disorder during any given year and more than 50 percent of Americans will suffer in their lifetime, statistics that are cause for serious concern.2 Further, the most recent studies show these trends have been worsening. For example, over the past two decades (prior to the COVID-19 pandemic), suicide rates in the United States increased by 35 percent overall.3 The prevalence of anxiety and depression has risen, with the most dramatic increases occurring in younger generations.4 These numbers may even underestimate the scope of the issue, because mental health problems remain stigmatized, and populations that are likely to have a high burden of mental disorders, such as people who are incarcerated or homeless, are often not included in epidemiologic studies.5 In addition, these studies largely assess clinically relevant levels of mental health disorders but do not capture levels of suffering from symptoms that do not meet criteria for clinical diagnosis. Such symptoms can still impose a significant burden, but they are obscured by the prevalence measures obtained within our scientific studies and surveys that typically query whether someone has a mental health disorder diagnosis. As a result, our current statistics likely fail to portray the full picture of mental health in the population. Most studies and surveillance activities also focus on manifest mental health disorders per se, not positive mental health at the other end of the spectrum. Among studies that do assess positive functioning, evidence suggests that emotional well-being (sometimes referred to as positive mental health, happiness, or flourishing) has also declined over time.6
The pandemic has made mental health a national priority.7 If there is any silver lining to these pandemic years, it may be the spotlight they have shone on long-standing challenges with which population mental health researchers have been grappling for decades: While increasing access to and improving mental health services is critical, the scope of the mental health crisis we face as a country far exceeds what can be fully addressed within the traditional medical system. Population-level approaches that prioritize prevention and fostering capacity for healthy functioning are urgently needed. However, there are major gaps in our understanding. A core issue is a lack of comprehensive insight into upstream structural factors that affect mental health. We have also failed to appreciate fully that while some conditions clearly contribute to worsening mental health (for example, extreme poverty), the simple absence of these conditions may not guarantee good mental health. Indeed, other conditions may also need to be in place (such as socially cohesive communities) to make it possible for a greater share of the population to experience emotional well-being.
A substantial body of research has already identified a range of circumstances contributing to higher rates of mental health problems including, most recently, the high levels of uncertainty and loss caused or exacerbated by the pandemic.8 Less work has identified strategies for addressing these conditions in ways that facilitate not only mitigation of harm in the moment but also sustained improvements for the long term. Thus, effort must be directed to identifying both harmful and health-promoting conditions as well as developing strategies for managing the distribution of these conditions throughout society. Key questions include: What are the social and environmental factors that promote emotional well-being and prevent development of mental illness at a population level? What factors should policy and practitioners target to shift the distribution of population mental health to healthier levels in both adults and youth in ways that are sustainable? What factors must be in play to protect mental health in the context of significant societal challenges? Are there specific resources or assets that are particularly potent for promoting population mental health?
The deeply troubling trends of worsening mental health have increased calls for greater attention to translating research findings into practice. On the plus side, the maturation of social epidemiology, the discipline that focuses on how social structural factors affect the distribution of health and well-being, over recent decades has shepherded the development of a set of robust tools that can help address the questions posed above.9 With sufficient investment of both human and financial capital, the scientific community and public health practitioners are well poised to address population mental health in meaningful and lasting ways.
In this essay, we review the mental health consequences of the pandemic in the context of prior trends, and discuss novel approaches for addressing gaps in our knowledge and practice. Among these approaches, we consider 1) different levels and timing of preventive strategies, 2) the often-overlooked connection between mental and physical health, 3) population-level interventions that address upstream social determinants of health, and 4) a greater focus on emotional well-being. While the terms “mental health” and “mental disorders” are broad, when considering mental health problems here, we are primarily focused on common mental disorders that include the categories of anxiety, depressive, and trauma-related disorders, according to the Diagnostic and Statistical Manual of Mental Disorders (DSM). Going forward, researchers will also want to consider a broad range of other disorders (for example, psychosis, eating disorders) as well.
The effects of the COVID-19 pandemic on mental health intensify troubling trends of declining emotional well-being that were already in play throughout the population before the pandemic. Multiple peer-reviewed studies have specifically demonstrated high rates of mental health problems that developed or were exacerbated with the onset of the pandemic, including depression and anxiety, in the United States and elsewhere. One meta-analysis of sixty-one longitudinal studies across the globe that compared mental health indicators before and during the pandemic found an overall increase in anxiety and depression in March–April 2020. Depression remained elevated in May–June 2020 while anxiety decreased on average.10 Another review estimated an overall global increase of 53.2 million cases of depression and 76.2 million cases of anxiety attributable to the pandemic.11
As the pandemic evolved in the United States, mental health estimates continued to change alongside infection trends. For example, the Household Pulse Survey, a rapid online survey distributed jointly by the Centers for Disease Control and Prevention and the U.S. Census Bureau, estimated that the proportion of adults showing symptoms of anxiety or depression increased from 36.4 percent in August 2020 to 41.5 percent in February 2021, based on a widely used screening questionnaire.12 Moreover, the proportion of adults reporting an unmet mental health care need increased from 9.2 percent to 11.7 percent during this time.13
Several subsets of the population have been particularly affected by mental health problems during the pandemic, including those who were already vulnerable, such as lower-income individuals more likely to lose employment during shutdowns, women who left the workforce to take on additional caregiving responsibilities at home, individuals with prepandemic mental and physical health problems, and those directly infected with COVID-19, particularly severe cases.14 Other vulnerable subsets of the population included children, adolescents, and young adults, many of whom lost access to their primary social networks due to school closures, remote classrooms, and disruptions to their daily routines and predictable structures.15 Importantly, mental health disparities may also have been exacerbated during this time. A recent report by the U.S. Surgeon General pointed out that Black, Latino, and Indigenous youth all had higher levels of mental health problems than white youth in 2020 and 2021, potentially due to their greater likelihood of losing a parent from COVID-19 and to the loss of crucial social networks in school.16LGBTQ+ youth and those with intellectual and developmental disabilities were also vulnerable, as many lost access to critical school-based services and support networks.17Rising mental health problems among younger people are of particular concern, given that such problems often persist across the life course and increase the risk of chronic disease and premature mortality in later years.
Psychiatric epidemiologist Bruce P. Dohrenwend and others have identified numerous characteristics of stressful and traumatic events that contribute to whether individuals will go on to develop high levels of distress and mental health problems.18 The pandemic fits the profile of a stressor likely to lead to more mental health problems in the United States. It is widespread through the community and has multiple components that are toxic for mental health. Such factors include not only fear of being directly infected with COVID-19, but also increased social isolation and confinement, bereavement, rising levels of stigma and discrimination, caregiving stress, and economic disruption. In fact, the pandemic fits into every one of Dohrenwend’s six posited characteristics of events that contribute to “uncontrollable negative changes” for most people.19 Specifically, it is an external and negative circumstance that is unpredictable, affects many aspects of people’s lives and functioning, has effects of high magnitude, and has the potential to exhaust individuals physically.20
Moreover, the COVID-19 pandemic affected populations worldwide. Few countries and individuals were untouched, limiting resources that could be made available to those in need. Further, unlike many other types of disasters, there were few places anyone, rich or poor, could go to feel safe. Thus, all people across the globe needed to manage a widespread sense of unsafety, which has long been recognized as a risk factor for poor mental health and, more recently, for poor physical health as well.21 In addition, unlike many large-scale stressors that occur within a confined time period but then remit (for example, extreme weather events), the pandemic has been both acute and ongoing; we do not know when it will end or if there will be a time at which we can say it is truly over.
We are at an inflection point. The attention the COVID-19 pandemic has brought to the mental health crisis in the United States offers an opportunity to broaden our thinking about mental health and ways to improve the troubling trends. Across public health and medicine, in the face of calls to address the high burden of mental disorders in the population, the most common responses include discussing barriers to mental health care, ways to improve access to evidence-based treatments, and how to increase funding for developing new treatments. These proposed strategies and solutions stem from the reality that many individuals with mental disorders never receive appropriate treatment—or suffer for years before they get treatment—and even among those who are able to access care, many fail to receive effective treatment.22 While it is critical to help those who are suffering, and indeed treatment has been transformed in important ways during the pandemic (for example, making telehealth much more accessible), such efforts are largely informed by the “medical model,” wherein treatment providers seek to detect and improve disease states. From a population health perspective, however, addressing problems with mental health treatment—even if done most effectively—will not be sufficient to decelerate or disrupt rising rates of mental health problems and thereby shift the distribution of population mental health meaningfully. Addressing problems with treatment focuses primarily on high-risk or already-impaired individuals, but this approach does not help to prevent declines in emotional well-being across the population.23
Efforts to promote mental health and emotional well-being will require not only identifying factors that increase the likelihood of attaining emotional well-being in the first place but also considering if these factors promote capacity to maintain emotional well-being in the face of large-scale stressors (that is, resilience).24 Moreover, we will need to go beyond considering factors at the individual level (for example, genetics or behaviors). To develop a comprehensive understanding of the forces that shape population mental health, we will need to examine the roles of community, social and physical environments, policy, and culture.25 Thus, we call for applying a population health lens to identify effective solutions for protecting and maintaining emotional well-being. COVID-19 as an infectious disease revealed that physical health is a public good (in other words, my health depends on the health of the people around me and on how they take care of their health). We must now recognize that mental health is also a public good. Moreover, addressing mental health at the population level will have downstream benefits for physical health.
A population health lens is not new by any means. In fact, many of the most dramatic public health improvements in the United States in the last century were achieved through population-level interventions. For example, decreases in vehicular deaths and lung cancer incidence were each largely driven by substantive changes in policies, laws, and improvements in technology, rather than by efforts to work with individuals one by one to change behaviors. However, for mental health, beyond issues of surveillance and treatment accessibility (that is, strategies focused on treatment of people with diagnosed disorders), a population-level approach to increasing the share of the population that attains and maintains emotional well-being has not been as widely implemented.26 We call for mental health research and practice to take on this challenge.
In both scholarship and among practitioners, mental health is often framed with respect to diagnoses (for example, generalized anxiety disorder or major depression), which lead to a binary view of mental health states, separating individuals into “healthy” or “sick” categories. Such designations are useful in medicine to communicate with insurers, to include in medical records, to distinguish when and which individuals need treatment, and to draw attention to high-risk individuals and populations. However, mental health ranges across a large spectrum, and far less attention has been given to the antecedents and consequences of states of emotional well-being at the healthiest end of the mental health spectrum.27 This perspective is highly congruent with the World Health Organization’s definition of health as “a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity.”28
To promote mental health effectively across the life course and in all segments of society, we must consider the full spectrum or distribution of mental health in a population when designing interventions, rather than focusing solely on those at highest risk. Such efforts would require monitoring, observing, and evaluating an inclusive range of mental health symptoms or states occurring in each population, from severe psychopathology at the unhealthiest end of the continuum to emotional well-being at the healthiest end. Greater appreciation of the full spectrum of mental health may suggest that a key goal for population mental health is not simply to reduce the number of people with psychopathology, but also to increase the number of those who have high levels of emotional well-being. This perspective may also provide an impetus for identifying novel targets for interventions and different approaches depending on whether one is aiming to reduce suffering at the bottom end of the spectrum or to improve functioning and well-being among all.
To improve overall population health and “shift the curve” of an entire population, different points of intervention are possible over time. We illustrate these potential points of intervention in Figure 1, showing a hypothetical trajectory or path of both mental and physical health over the life course for one person, for simplicity. In this case, the path includes both remission and relapse of mental health problems. But it is important to note that many different trajectories are possible.
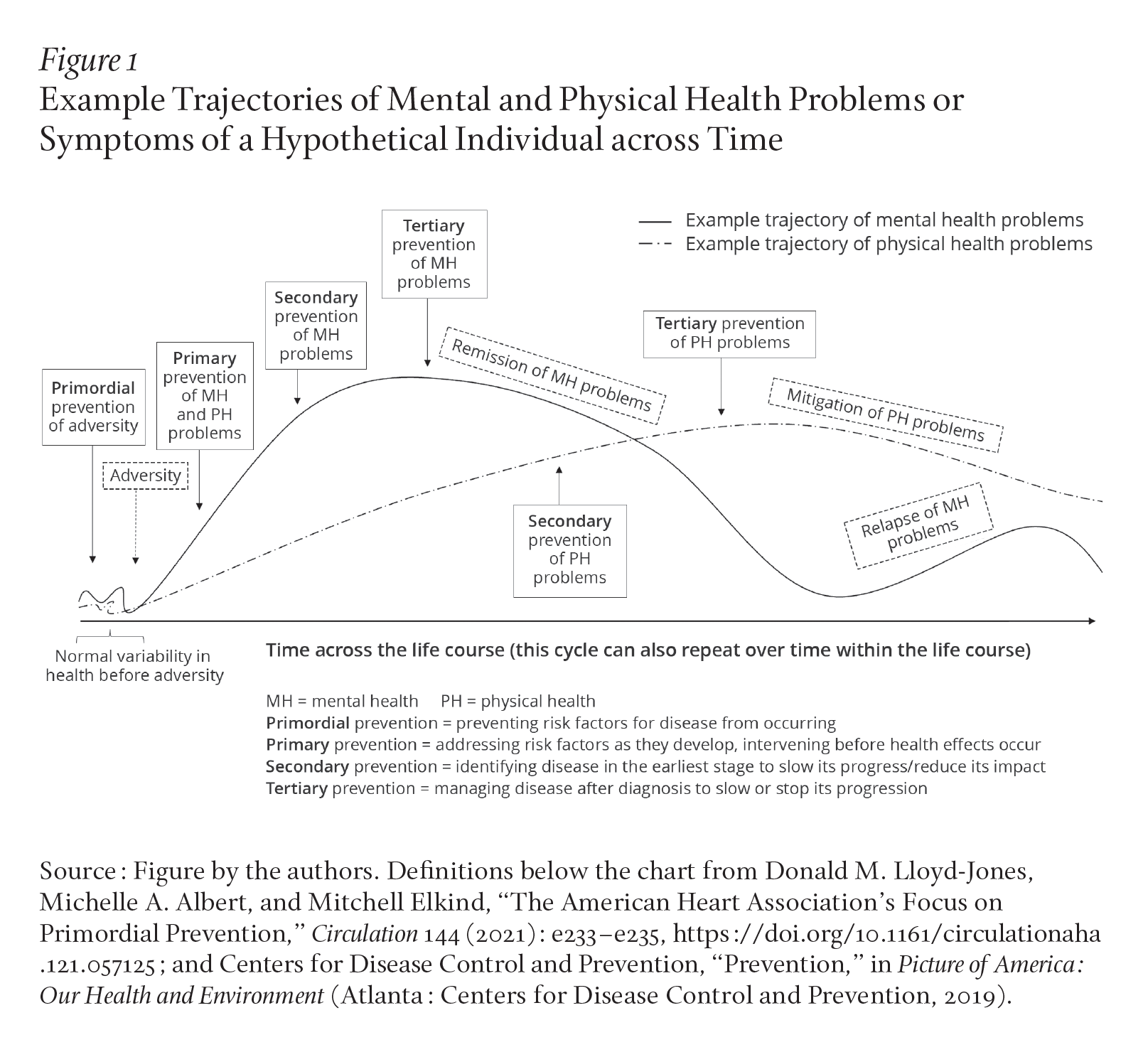
The solid boxes depict different potential interventions, each of which can be implemented at either the individual or population level. We argue that, where feasible, 1) population-level interventions may be more effective for influencing overall population health than individual-level interventions, even when the latter are implemented at scale, and 2) intervening prior to the development of manifest disorder and earlier in the life course is more likely to promote greater prevalence of emotional well-being in the population over time. Another advantage of implementing population-level interventions relatively earlier in the life course is that they may promote increased resilience: populations and individuals with better initial mental health or emotional well-being may confront trauma and adversity (which will inevitably come up throughout the life course) more effectively. Shifting the overall distribution of mental health may result in a more resilient population overall.
Prior work has defined various types of prevention or intervention strategies depending on their primary targets within the trajectory of an individual’s mental health experience. “Primordial” prevention strategies, which aim to prevent risk factors for disease from occurring, have been widely applied as a component of larger efforts to reduce the population burden of cardiovascular disease, but less so in relation to mental health disorders.29 Considering whether (and which) primordial prevention strategies will improve population mental health may provide valuable insight when developing novel protocols and timelines for prevention and intervention activities. As depicted in Figure 1, primordial prevention in the context of mental health could correspond to efforts to prevent (or limit) exposure to adversity, a type of experience that has been shown to increase the risk of a range of mental disorders.30 At the population level, an example could be climate-change initiatives that have the potential to prevent natural disasters from occurring, which in turn may reduce the levels of new-onset post-traumatic stress disorder (PTSD) across the population. In contrast, at the individual level, trauma prevention might include self-defense and safety training aimed at reducing the risk of assault, or parenting interventions aimed at reducing the risk of child abuse.
Despite applying primordial prevention strategies where possible, adversity in some form will inevitably occur for many people (for example, job loss or the death of a loved one).31 Although we cannot reverse a past trauma or initial symptom reactions, we can intervene as early as possible after a traumatic or adverse event, which would be considered “primary prevention” of mental or physical health problems.32 Examples at the individual level include initiatives like Psychological First Aid, which is a modular approach that can be administered to people immediately following traumatic events.33 At the population level, primary prevention might involve administering a stepped care intervention approach delivered to communities as a whole that are affected by a mass shooting or natural disaster.34 This type of approach includes both low- and high-intensity interventions in turn, and can be tailored across groups depending on the intervention response.35
“Secondary prevention” is defined by identifying disease in the earliest stage to slow its progress or reduce its impact. An example of individual-level secondary prevention in the context of mental health could be to initiate early treatment among individuals experiencing mental health problems, whereas a population-level secondary prevention strategy for improving mental health could be regular screenings for mental health problems for all primary care patients, as part of routine medical care. This strategy may become more commonplace in the future, as the U.S. Preventive Services Task Force recently released draft guidance that all adults be regularly screened for depression and suicide risk, a promising step forward for population mental health.36
Finally, “tertiary prevention,” which corresponds to managing disease after diagnosis to slow or stop its progression, applies to patients with manifest psychiatric disorders in the context of mental health. Tertiary prevention usually occurs at the individual level (that is, medical treatment in its most common form), but we can also conceive of this type of preventive activity as occurring at the population level. Examples might include application of the American Disability Act or medical leave policies that ensure that employees with mental disorders receive appropriate accommodations, such as being able to access treatment when they need it, without losing their jobs.
As demonstrated in painful detail throughout the pandemic, mental disorders and distress cause suffering in themselves. However, they also have a “long arm,” as they are linked to long-term adverse physical health outcomes, including common chronic diseases that are leading causes of death.37 For example, many mental health conditions are associated with an increased risk of cardiovascular disease, which remains the most common cause of death in the United States.38 As highlighted in a recent statement by the American Heart Association, there is now a greater appreciation for the relationship between mental health and cardiovascular disease.39 Multiple prospective studies, which follow individuals over time, have found that in women, PTSD increases the risk of later developing cardiovascular disease.40 Other equally rigorous studies have shown similar findings in men. Importantly, more common disorders like depression and anxiety are also strongly associated with an increased risk of subsequently developing cardiovascular disease and other physical health outcomes, including autoimmune diseases, cancer, cognitive impairment, and frailty.41 Even subclinical levels of psychological distress can increase the risk of adverse physical health outcomes, with numerous studies showing these effects on cardiovascular disease, arthritis, and diabetes, among others.42 Thus, our hypothetical trajectory illustrated in Figure 1 further considers how interventions to improve population mental health may also affect subsequent physical health and even earlier mortality.
Emerging evidence suggests that if we effectively treat mental disorders, we may be able to mitigate physical health sequelae—as depicted in Figure 1—although the findings to date remain somewhat limited. For example, one study from our group found the relationship between severe PTSD symptoms and the risk of developing cardiovascular disease in a large group of women was weaker among respondents whose PTSD symptoms had remitted or lessened over time.43 Another study of male veterans found that although there was a relationship between current PTSD severity and heart rate variability (a marker of cardiovascular disease risk), there was no relationship between remitted PTSD symptoms and heart rate variability.44 Taken together, these findings suggest that at least some physical health sequelae associated with mental health problems may be mitigated when underlying mental health problems are alleviated or remit. At the same time, a recent systematic review of the literature concluded that while cardiovascular or metabolic risk markers and conditions may be improved with mental health treatment, some longer-term biological alterations underlying manifest cardiovascular disease may be too far along to reverse.45 Therefore, it is important to consider earlier promotion of mental health (closer to the left side of the timeline in Figure 1) before mental health problems are established and treatment is necessary.
Given 1) the strong connection between mental and physical health and 2) the widespread mental health problems during the COVID-19 pandemic, it follows that many people in the United States and globally may experience adverse physical health sequelae in the next few decades. Once physical health conditions like heart disease begin, limiting their progression (that is, secondary prevention) can be challenging.46 This cascade of events could impose an even higher societal cost than may now be evident in the evolution of the pandemic. Thus, the need to invest in strategies to improve population mental health is even more urgent than an examination of mental health statistics alone might suggest.
Moving beyond the theoretical, how do we apply our model of early prevention and intervention at the population level in practice? We will need to consider strategies that enable individuals to attain emotional well-being in the first place, as well as those that make it more likely that people can maintain emotional well-being in the context of significant challenges. How, then, might we address large-scale emergencies like pandemics in addition to everyday stressors and adversity? While preventing trauma from occurring in the first place is a laudable goal, the reality is that experiencing trauma will be unavoidable for many people in their lifetimes.47 So, when adversity does occur, how do we disrupt the downstream consequences, including both mental and physical health problems, applying principles of primordial and primary prevention as illustrated in Figure 1?
To answer this, we can consider policies and practices developed in other disciplines and sectors—from education to transportation to finance—given clear evidence that these factors shape the capacity of individuals and communities to attain and maintain health. For example, economic policies, which have the potential to alter many aspects of people’s lives while also narrowing economic inequalities, may provide promising directions for relevant population-level mental health interventions. The connection between income and health has long been understood, and some rigorously designed studies have further demonstrated that economic interventions can lead to improved mental health specifically. As one illustration, many studies have shown the benefits of cash transfers for reducing mental health problems and increasing emotional well-being in a variety of contexts.48 Importantly, several income policies put in place during the COVID-19 pandemic show promise for driving large-scale mental health improvements. For example, one study examined mental health in the wake of implementing income-support policies. Data on millions of calls to the National Suicide Prevention Lifeline were collected across nineteen different countries from 2019 through early 2021. The data showed that although calls initially increased at the beginning of the pandemic, they decreased in the United States after the income-support policies were administered, even accounting for changing COVID-19 infection rates.49 Income-related interventions also have the potential to prevent new trauma or adversity from occurring, serving as a primordial prevention strategy according to our model. For instance, more income can prevent home foreclosure, and foreclosure has been shown to increase incidences of anxiety and depression.50
Other policies may also be considered as population-level primordial prevention strategies. Prior work points to the promise of family leave policies. For example, one large-scale European study of older women linked decades of maternity leave legislation data to self-reported mental health outcomes. The findings were striking, whereby women who were given more generous maternity leave during the critical period of their first child’s birth reported fewer depression symptoms later in life, compared to those who were not given generous leave.51 Workplace policies may also be relevant, given the substantial body of research suggesting the workplace is a critical determinant of population health and emotional well-being. In recent studies, specific work conditions that influence worker mental health have been identified, such as one’s schedule and the level of control over one’s work.52 Based on these findings, researchers have proposed strategies employers and institutions can use not only to reduce mental health problems but also to promote greater emotional well-being.53 Such strategies include increasing workers’ control over their work schedules, giving workers more voice in their organizations, and providing training and support for employers to promote stronger social relations at work. This area of intervention may be especially relevant during and after the COVID-19 pandemic, which changed the face of work in many ways and led several types of organizations to view employee health as more critical.
Recent work has also suggested that engagement in the arts, and policies that make the arts more accessible, may be another primordial or primary prevention strategy. A recent scoping review showed that engagement in the arts can promote both mental and physical health.54 Numerous studies demonstrate that art can affect mental health directly as well as indirectly through encouraging health-promoting behaviors and supporting child development. For example, one study found that older adults who more frequently engaged in cultural activities, such as attending museums, theater, or cinema, had significantly less depression across ten years of follow-up than those with less frequent cultural engagement.55
For primary prevention (such as intervening after adversity occurs), we might consider ways to embed strategies that can disrupt potentially harmful effects of trauma or adversity into community (at schools, for instance), organizational (in the workplace or other institutions), and health care systems. For example, intervening with social support (both formal and informal) after trauma or adversity occurs appears to lead to better mental health, and perhaps to better subsequent physical health as well. Prior work suggests that such effects can even reach across generations. In a recent study, among women who reported high levels of adversity in childhood, different types of social support during pregnancy (such as receiving material aid or having companionship) buffered against potentially toxic effects of their early experiences of adversity on the fetal growth in their offspring.56 Findings from the disaster literature have also illustrated potential benefits of related factors like social engagement for mental health. For example, a natural experiment study after the 2011 Tōhoku earthquake and tsunami found that higher community-level social engagement was associated with lower odds of PTSD among affected older adults.57
In addition to identifying broad determinants of health as targets for primordial or primary prevention and intervention, secondary prevention strategies that intervene more directly on mental health may also be valuable, with the potential to interrupt downstream effects of poor mental health (such as poor physical health, as shown in Figure 1, and even the prospect of earlier mortality). While it can often be difficult to intervene on individual mental health at scale, the Psychological Science Accelerator, a network of researchers that seek to facilitate crowdsourced research projects, has made it possible to implement and evaluate the use of evidence-based interventions at the population level.58 As one example, a pandemic-specific online mental health intervention developed for large-scale implementation across multiple countries involved reappraisal, an emotion-regulation strategy aimed at modifying how individuals think about a given situation.59 Through the Psychological Science Accelerator, researchers conducted an online randomized controlled trial to evaluate if a reappraisal intervention would lead to better mental health. Over twenty-one thousand participants were randomly assigned to one of two reappraisal interventions designed to change emotional responses to stressful situations. One reappraisal condition was “reconstrual,” which involves trying to alter how a stressful situation (in this case, the pandemic) is mentally represented or construed. The second reappraisal condition was “repurposing,” which involves trying to focus on positive outcomes that could arise from a stressful situation.60 In addition to these two reappraisal interventions, participants could also be assigned to one of two control conditions: active or passive. The active control condition instructed participants simply to reflect on their thoughts and feelings. This study found that participants in both reappraisal conditions had less negative emotion and more positive emotion than their counterparts in the control conditions. This suggests the potential utility of scalable, low-cost digital interventions that could be applied across the globe among those willing to engage in this type of activity.
Another secondary prevention strategy was developed in the Laboratory for Youth Mental Health.61 Targeted at younger individuals specifically, this protocol relies on brief digital interventions designed to help children with mild to moderate mental health concerns improve their coping mechanisms, including a recent one designed specifically for the pandemic.62 These types of nonclinical interventions targeting populations who are not yet in the highest-risk groups can reduce the overall demand for more in-depth clinical or professional services, ideally making it easier for those who have a higher need of clinical services to access them. Such strategies may be particularly relevant during large-scale events like the pandemic, which affect the availability of care. Furthermore, increasing availability of technology in recent decades has made digital mental health interventions in general a promising avenue, reaching large numbers of people.63
Finally, a variety of psychological interventions have been demonstrated to support and improve states of emotional well-being before trauma or adversity even occurs, intervening directly on mental health well-being rather than on a risk factor like adversity. A recent systematic review and meta-analysis of over four hundred psychological interventions to improve emotional well-being in a range of populations found support for mindfulness-based and multicomponent positive psychological interventions both inside and outside of clinic settings: that is, among both healthy and sick populations.64 Key elements of such strategies may be scalable if they were routinely included in various education or workplace settings in relatively healthy populations.
It is promising that the importance of mental health has been more readily recognized and appreciated as part of the reaction to the COVID-19 pandemic. Illustrating this point, the U.S. Surgeon General recently declared mental health a national priority, particularly among youth.65 However, many more steps can and should be taken to address our current mental health crisis more comprehensively, including making more funding available for research and practice. Research funding has historically skewed toward treatment, not prevention, and even within research focused on prevention, there is often an individual-level focus. We argue for the need to prioritize population-level work, including efforts to rigorously evaluate existing large-scale interventions (for example, the COVID-19 stimulus package).
Funding for this type of work will likely require political will and government support, which could be in the form of a national call for research and action toward mental health promotion, similar to past calls for action around topics like the health effects of climate change and the conflicts in Iraq and Afghanistan.66 We need a similar large-scale investment to address current trends in population mental health, made more prominent by the COVID-19 pandemic. Ideally, such investment will include research that considers the full spectrum of mental health and leverages all we have learned about how the social and physical environment and circumstances in which people are born, live, and work alter the population distribution of mental health problems and emotional well-being. We have seen massive acceleration and success in other areas when the scientific community decides something is truly a priority worth investing in (such as the COVID-19 vaccines, genetics research, and the opioid epidemic). We believe the same can be done for mental health and well-being promotion.
Ultimately, a population health lens on mental health calls for an interdisciplinary approach, identifying how and when policies and practices from diverse sectors, including housing, education, urban design, economics, medicine, and law, might affect population mental health. Any new interventions we design must be both durable in their effects and scalable, with efficacy and reach across a variety of populations. Changes in exposures that may have small individual effects, but that ultimately affect a sizeable number of people (like economic policies), can have a very large impact on population health overall.67 Interventions can also be targeted at the school, workplace, or other organizational levels to attain a wider reach.
In sum, we believe that a population-level, interdisciplinary approach focused on early prevention is needed in fields involved in mental health research and practice, including psychiatry, psychiatric epidemiology, psychology, social work, and medicine. These shifts in perspective may help address the near-term health effects of the COVID-19 pandemic, and improve population health, including both physical and mental health, for generations to come.